General EEG Collection
In the TQ guide we recommend that assessments be recorded before 11am.
The assessment gives the trainer a starting place. I know what NOT to aim at, and have some ideas as to where and what seems to be a “bad energy habit” that might be resulting in states and behaviors that the client would like to change. But with all that, I can’t with any degree of certainty say which protocol is going to make the change until I’ve tried them and seen how the client (not necessarily the EEG) responded.
Electrodes and Electrode Placement
It’s never a good idea to mix electrodes–certainly not metals. Ideally use electrodes that are all about the same age and degree of use to minimize offset.
Ground
The function of the ground electrode is to help avoid overloading the amplifier if you should have a static discharge or some other powerful signal. The ground gives the signal a way to get off the body other than through the amplifier’s circuits. It is also used as a comparison for the active(s) and reference(s). The amplifier uses “common-mode rejection”–canceling out any signal that appears in all sites–as a way of removing background noise.
The ground can be placed anywhere on the client’s body, but the quality of the connection will be affected by the quality of the connection of the ground (as with all other electrodes). Ideally the ground would be on a site equidistant from the two active sites, but it’s not critical. It can be anywhere on the head, back of the neck, behind an ear or on the earlobe or even (with certain systems) on the client’s wrist.
References
One of the basic rules is that, if you are using an ear reference, place it on the same side as your head lead. Thus C4/A2 is correct and C3/A1 is correct.
Jumpers
You have to use linked references or the assessment and any synchrony training. A jumper can be used for this. You should not use the jumper between a reference and a ground–only between two references. The Optima+, Q-wiz and U-wiz can link references without a jumper.
Good Signals
You should be able to see if you have a trainable signal or not with a quick look at the oscilloscope and power spectrum. With modern amplifiers, the old “standard” of below 10 kohms for training, below 5 for research is essentially meaningless. I learned long ago that lead placement is technique, technique, technique. Prep each spot lightly for 10 seconds, put a mound of paste over the electrode head and make sure it is in contact at least some of it with scalp, and impedances are consistently low. The real benefit of the impedance meter that I used in the past was that it measured offset between electrodes. There again, if you work with groups of electrodes that were purchased at the same time, same type and same material, it is super-rare to run into offset issues.
Bald heads have tougher skin, so I usually prep more than usual. You don’t have to shave a bare spot on the head to get a good connection. I’ve worked with a few clients with remarkably thick (densely populated) hair where it was difficult to get to the scalp, but even with those it was not a major issue.
If you have extremely dense hair, where you simply can’t spread in away from a spot of scalp and get a space of clear scalp that is visible, using combs or bobby pins or such to part the hair away from the site will usually help hold it away. As has also been suggested previously, if you can get the scalp visible, a small dab of Ten/20 paste lightly rubbed into the scalp at that site will usually help give good connections AND help hold the hair. I go for a “starburst” pattern if I do that, so the hair spreads away from the open area in all directions. Then use a blob of paste that fills the electrode surface or cup and mounds up so that one could fill a second electrode facing the opposite direction with the mound. Place the tip of the mound on that small area of clear scalp and lightly “wiggle” the electrode down and into place so it is sitting on a pad of paste.
Many people do prefer the saline system for a couple reasons. First, it is often used without prepping, though I would recommend prepping even using this system. Second, you are pushing (actually holding with the head apparatus) the edge of an electrode encased in some kind of material that keeps it wet with saline solution against the scalp. A much smaller bit of scalp will work. Third, the saline solution, like any water, flows through hair and makes contact with the scalp, so getting a good conductive path from scalp to electrode is easier.
More paste shouldn’t give you better but worse connections. When you have giant globs of paste in the client’s hair, you are creating a lovely little antenna to pick up signals from the environment.
An electrode does pick up activity from a circle with an area of about 6 cm2 with the center of the electrode as the center of a circle, because the bone tends to “smear” the electrical signal a bit (it’s not a very good conductor of electricity). And in a monopolar (referential) or bipolar (sequential) montage, you are indeed measuring between the two (active and reference) electrodes.
But what is it we are measuring? It’s not amps (flow of current) but voltage (the difference in electrical potential that “drives” electrons from the more activated to the less activated site.) You can’t have voltage at one site. Voltage is a comparison value between two sites. But it’s not exactly measured AT the two sites. It’s measured BETWEEN them. If you could stand at the Active electrode and look toward the reference electrode, and at the same time could stand at the reference and look toward the active electrode, you would only see about 30% of the EEG signals between them: those that were primarily lined up between the electrodes and fairly close to one or the other electrodes.
So it does matter where you put the reference. If you measure from Cz to A1, you’ll be looking over the left hemisphere; if you change your reference to A2, you’ll be looking over the right hemisphere. And remember that, although we SAY that the earlobes are inert sites, we know that, in fact, each does have a signal that is picked up from the field emanating from the temporal lobe. Since the temporals are often quite different in signal, the ears also can be quite different.
Signal issues
There are two places you can look to see if your signal is decent (meaning probably that you have good connections) or not.
The Oscilloscope should show a fine single line for each signal included in it that cycles back and forth across the baseline and it should show variability–not a highly regular, mechanical-looking waveform.
The Power Spectrum should show the amplitudes (height of the bars) for all frequencies (they’re listed across the bottom of the screen in this design), and they too should be fluidly changing. The one thing you must look for is a huge spike at 60 Hz if you are in a country that has a 60 Hz electrical system like the US or at 50Hz if you are in a country with a 50 Hz signal.
If you start a minute of recording and immediately see it is bad, click Pause. Fix the electrodes then start again. It’s easy enough to remove bad signal if it does not continue beyond a few seconds. The assessment requires a minimum of 50% good data.
I always ask clients to let their mouths hang open during the measurements, so they cannot tense the jaw muscles.
Sync Errors
Sync errors are shown when something interferes momentarily between an amplifier and the computer or the amplifier and receiver/dongle. They are more common in wireless amps. Often it means someone put an arm or other body part between the two units. They should be able to “see” each other at all times for ideal signal processing. A brief blink on of the Sync Error notification is not a problem. If it stays on, training data may be lost.
Activation Tasks for Collection
Frontal Sites
Digit span (series of one-digit numbers given with 1 second between each) with client repeating accurately; do 30-40 seconds forward tasks and finish the last 20-30 seconds asking the client to repeat in reverse order. I do both digit span and reverse digit span in one minute to determine both working memory and divided attention memory. I don’t know the norms, except that we are usually looking for around 7 as reasonable performance, but I can track how many a client did and can easily re-run the process at the end of a session, often showing positive change.
To create the digit span, simply write down a series of one-digit numbers (e.g. 6…4…3…9…1). Create sets of 3, 4, 5, 6 and 7 numbers. Then for home training, whoever is helping with your assessment can read them off, starting perhaps with 4 or 5 digits–one second between each–and verify that you are giving them back in order. You can use the same set for forwards and backwards. To create the serial calculations, same thing. Just write down some calculations ranging from less to more complicated and let the person who is helping read them to you and verify your answer.
Central Sites
Read silently, be prepared to answer questions about details in the material AFTER completing the data collection.
Parietal Sites
Serial calculation; give a series of skill-appropriate calculations which build on one-another (e.g. 2 times 3…times 4…divided by 6…the answer would be 4) I do the serial calculation verbally and tell them to perform each calculation as I give it to them and give me the answer only when I stop. So I might say 2 plus 3…times 4…divided by 6. The idea is to start with tasks the client is quite likely to succeed with and then increase the difficulty based on the client’s success. I don’t try to make the client feel stupid but do try to get a sense of where the failure point is. I suppose, if you had a client about whose auditory processing you had serious questions, you could do a series of visual steps ala flash cards (e.g. “2+3”, “X4”, “/5”).
Temporal Sites
Listen to spoken or read material, paying attention to details. Ask questions about the material AFTER completing the data collection.
Midline Sites
Give the client written material and ask him/her to find a specific combination of letters (you may use something like Where’s Waldo with young child) such as t, h and e in order, which may appear alone or as a part of another word. Client counts the number of appearances silently.
Optional Sites
As I recall the ones in the instructions:
fpz/cz and Fp1/Fp2 (sorting task, often with regular playing cards, more or less complex depending on the client)
F7/F8 reading aloud
T5/T6 reading silently
The tasks I do are less normed but they give me the capacity to push people to a challenge point. For example, 3 minutes of simple math problems would not necessarily produce activation in an engineer, whereas my serial test allows me to start easy and increase the difficulty (of calculation or the length of the sequence) to get to a point where some kind of activation is required.
Tasks for a Nonverbal Client
Assuming that by “non-verbal” you mean not speaking or writing–not that the client is unable to understand verbal material, I’ve used the following, but anything would work:
Digit span: holding up a series of fingers, like catcher’s signals, and having client repeat them
Reading: I’ve used a set of words on a page, speaking one and asking the client to point to it; if that’s not feasible, do what comes to you. The central strip is not really a reading area, so you can do any general activation task.
Calculation: your idea is good (adapt the serial calculation using blocks and a number-board for answers, etc.)
Listening: again, I would tell a story and then ask the client to point to pictures or numbers to answer questions about it.
Visual task: where’s Waldo is one I’ve used with lots of kids, or the puzzles in Highlights.
Remember that it is more what the brain is doing during the task that is important than how well the client “performs” on the test.
Assessing a Blind Client
I’ve done an assessment of a person with seriously compromised vision, but he could still see light and vague shapes. I have absolutely no idea what to expect in terms of alpha blocking from eyes closed to eyes open tasks. It is presumed to be the data coming into the visual cortex that causes alpha to block, and in a completely blind person, that obviously would not happen. That could either result in no increase in alpha with eyes open (because the client is always aware using those senses) or no blocking of alpha when they are opened.
As for the tasks, you could substitute any language task for the Central strip reading (e.g. reading aloud to her), but the idea of reading with braille is a good one too. Regardless of how the information is coming in, the language areas should be activated. The pattern recognition (midline) task will be a much harder one. Here again, I guess you could ask her to find certain word or letter combinations, but we won’t really be seeing the visual cortex activate for that in any case.
Assessing a Client with Significant Brain Damage
Time to drag out your creativity glasses.
I’ve done several assessments with folks whose brains were seriously compromised. Usually we’ve been able to find tasks somewhat in the same range as the ones in the assessment. I’ve had people listen to a digit or two, then show the numbers of fingers or point at numbers on a page of the 10 digits to “repeat” them, do simple one-digit additions and point to answers, etc.
If they can’t do any of this type of thing, then I would simply have someone stand in their field of vision and talk to them, explaining something and gesturing–anything to try to see if the brain can activate (and how it does so) when a cognitive task is required. You might be surprised.
Certainly it’s possible to just do the heads page and gather just two minutes of data to see what happens, but it’s worth a little effort to get the third, if possible.
Assessing a Very Young Child
Generally I wouln’t even try to do an assessment on a 5-year-old. Their ability to sit quietly even for 15-20 minutes is very limited. Usually I would just have the parents complete the Client Report. You can load that into the TQ7 without loading any EEG data, and it will still give you a plan. If the child is very calm, go ahead and do the assessment, but just do EC and EO, and maybe skip the 5th step of the assessment, so you only do the first four, which will give you the info you need.
Repeating the assessment –
Should results change after training
Sure. If brains were neat mechanistic systems (as psychology assumes) rather than complex chaotic systems, that would work great. We need to understand that the “normative” databases used in population-based QEEG’s–and hence in most of the research that has produced the patterns we identify–are based on the assumption that brain measures produce what statistics calls normal distributions. But chaos theory tells us that this is not the case in chaotic systems. Each such system is completely unique, self-referential and self-reinforcing, dependent on its initial conditions. In short, EVERY chaotic system is perfectly “normal” given the conditions that led to its formation.
“A complex system is a system composed of many components which may interact with each other. In many cases it is useful to represent such a system as a network where the nodes represent the components and the links their interactions.” Sounds a lot like a brain, doesn’t it–or an ecology or weather system or economy–all systems which are notoriously difficult to “model” and control (at least if you expect your models to produce estimates that are anywhere near the actual results of the system.
The idea of whole-brain training is not that if we can just change a variable or two by feeding back information about it, the brain will neatly make a change in that variable and BINGO, we’ve succeeded. Rather we use the assessment to identify variables that are correlated with systems that demonstrate certain tendencies (e.g. anxiety, internal focus or peak performance). Hopefully we all understand that correlation does not equal causation. In other words, a fast right-rear quadrant doesn’t “cause” anxiety or terminal insomnia–nor do they cause a brain to have a fast right-rear quadrant. They often co-exist[, but likely both are related to other factors, some perhaps we cannot even measure.
Our goal is not to identify the levers to use to make the brain do more what we want it to. Rather it is to disturb the brain’s habit patterns in multiple ways by applying feedback–the main driver of complex chaotic systems. Ideally these multiple nudges result in the whole system (the homeostasis) shifting in a desired direction and establishing a new stable range of operation. Whether that means that all the measures we trained will change or not is problematic.
My position has been since my early days trying to convince people to let me put wires on their heads and mess around with electricity (before neurofeedback was something anyone had heard of) I don’t care if the Theta/Beta ratio changes or not. I care if the client can pay attention more effectively. And in most cases, unless there is an engineer or accountant parent, the client couldn’t care less about the ratio if the teacher or boss or spouse stops complaining, or if work can be done faster and more easily. Of course “scientists” and left-hemisphere thinkers who cannot accept experience as meaningful MUST have something to measure, choosing to ignore the famous dictum: Not everything that can be counted counts. Not everything that counts can be counted.
TQ – The Trainer’s Q
QEEG just means quantitative EEG. That involves digital (rather than analog) recording of the EEG from 18-128 sites, usually at least with eyes closed and eyes open, though often also at task. Data should have artifacts removed (signals that appear in the EEG but do not originate in the brain, like eyeblinks, electrical interference, etc.) The data are then presented in various views that allow the brain to be described in terms of frequency, amplitude/magnitude (power), variability and connectivity–the primary measures of brain function. In most cases the data are recorded using an electrocap, though individual electrodes can be used. The recording should be completed within 20-30 minutes so that brain activation is consistent throughout.
There are amplifiers with 19, 24 and more channels that allow all data to be recorded at once, and other systems that use amplifiers with 2 o4 4 channels that gather it serially with minimal delay.
The QEEG was essentially developed as a research tool, and the design of what most people think of as a Q is based on that approach. Q’s have been used by a number of researchers over the past decade or two to compare sub-groups of the population with specific problems against the population as a whole to generate pattern analyses that define ways in which people in the sub-group reliably differ from the population as a whole (e.g. how do the brains of anxious people tend to differ?)
The TQ7 uses an Electro-Cap and gathers eyes-closed, eyes-open and task data from the standard 20 EEG sites in about 20 minutes 4 channels at a time. It removes artifact from the data and presents standard maps, graphs and tables of brain EEG data in amplitude/frequency, symmetry, synchrony/connectivity, and variability. That’s a quantitative EEG.
The differentiation is, as you note, in how the data are used. There are “population-based” analyses, which compare the individual brain against a database of people and use z-score analysis to identify all the measures in which the individual differs by a certain number of standard deviations from the average of the population. For research this is perhaps helpful (though it is more likely to be used–because of the greater statistical validity–to compare sub-groups of the population against the population rather than one individual vs the population). From the trainer’s perspective it makes the significant assumptions that a) all deviations from the mean are negative and should be trained; and b) that clients want to be “average” in every way. From a researcher’s point of view using pattern analysis, this may be very useful. From a trainer’s it’s probably not. Z-score training doesn’t distinguish, in the words of Jay Gunkelman, between a broken leg and a crutch. Both deviate from “average”. As would the brain of Einstein, or a person with special talents in music or math or any other area.
The TQ7 is a “Trainer’s Q”. It uses the data descriptively instead of “normatively”. It uses a “Pattern-based” analysis seeks to identify those patterns which have been defined in QEEG research and empirically as relating to specific types of problems. The Population Q tends to gather data at a level of detail that is not generally very useful to trainers. For example, we know that alpha or theta can be divided into “slow” and “fast” bands (4-6, 6-8, 8-10 and 10-12 Hz). These relate to specific differences in perception and performance. However, outside of research, there’s no real benefit to looking at 4, 5, 6, 7, 8, etc Hz bands as the population Q does. So while we do have users who do research using the TQ7 (on training approaches), the QEEG is probably better fitted to that; and while there are folks who use the population Q to do training plans, I would argue that the TQ7 is better fitted for that.
Showing Clients Assessments
I don’t usually give them the assessment at all. I sit down and explain the Training Plan and the Training Objectives and that’s it. The rest is unnecessary and often confusing and frequently causes you no end of headaches when you start to get folks wanting to see how the numbers have changed (which they may or may not.) The assessment is for YOU, to guide YOU in preparing a plan to get them where they want to be. Keep their attention focused on the real-world changes and accurately reporting progress on same.
Collection
You can’t just record one set of sites a few days after recording the rest and slip them into the assessment. The brain changes hourly at least in terms of activation levels, etc. The closer together the sites are recorded, the better.
Fp1 and Fp2 are difficult sites to assess because they are prone not only to eyeblink but also to movement of forehead muscles. I would suggest you have the client bring in a cool sweat band and, after placing the electrodes, place the sweat band around the head to hold them in place.
In all 3 conditions, you need to stress to the client the importance of really focusing on keeping his/her forehead relaxed and, if possible, looking down during the eyes open and task conditions. That will minimize blinks.
Blinking during Assessments
Whenever you blink, your eye muscles produce large electrical signals, which can be picked up by the electrodes–especially those which are nearer the front of the head. These are called artifacts, since they appear in the EEG but are not coming from the brain. So F3 and F4, Fp1 and Fp2, F7 and F8 and Fz are all likely to be affected. In some people, the C and T sites can also show these big slow-wave artifacts which skew the EEG data.
So at least anytime you have electrodes in any of the above areas (and, if the client doesn’t have problems with the “peeking”, there’s no reason not to do it at all sites), you should peek in the eyes open condition and, if possible, in the task condition. Tasks are always done eyes open. So digit-span can easily be done peeking. Listening and calculation as well. Of course reading and pattern recognition tasks probably require eyes fully open.
Artifacting
Let’s clarify just for a moment the concept of artifacting.
When we do an assessment, we need to see the client’s brain data as completely and accurately as possible with as little as possible of non-brain electrical activity as possible leaking in. As you probably know, when recording toward the front of the head (though it can appear as far back as the parietals if a client is wearing contact lenses) the electrical signals produced by each eyeball and the muscles that blink and move the eyes appear as slow-wave activity in the EEG, and they are so much larger than brain signals that they can “swamp” the EEG reading. Especially around the temporal lobes, the masseter muscles used for chewing (and often a location where people hold tension) among others in the neck, face and head, can also produce strong electrical signals that appear as fast-wave activity in the EEG.
One of the most important things to understand is that the best artifacting is done while RECORDING the assessment. In order to have a reasonable chance of getting good brain information, we need at least 30 seconds of data (50% of the 60 seconds recorded for each minute). While it’s possible to remove some kinds of encapsulated artifact (like an eye blink or a movement), muscular tension or electromagnetic interference can be a constant presence which is impossible to remove. With practice you can recognize eye artifacts by looking at the power spectrum or the oscilloscope. A surge of all frequencies in both channels that raises amplitudes in frequencies below 6 Hz is almost certainly artifact. Oscilloscope tracings show a large wave form that looks like an “S” tipped on its side. A sharp surge in ALL frequencies–especially visible above 20 Hz or so–can indicate bracing or clenching of muscles in the power spectrum, and the oscilloscope shows very condensed and sharp waves.
There are also graphs on the trainer’s window to help identify fast or slow artifact bursts.
Getting the client to sit comfortably, with both feet flat on the floor (use a little footstool for short legs so they don’t hang) is very important. If necessary, do a little relaxation with the client before starting the recording. I usually ask the client to let his mouth hang slightly open so he doesn’t clench his teeth. When recording frontal sites with EO or at task, have the client keep his head up but look down at the floor in front of his feet. This keeps the eyes partially closed so they don’t try out quickly, and blinks tend to be less constant and very small. Most of the tasks can be done this way as well.
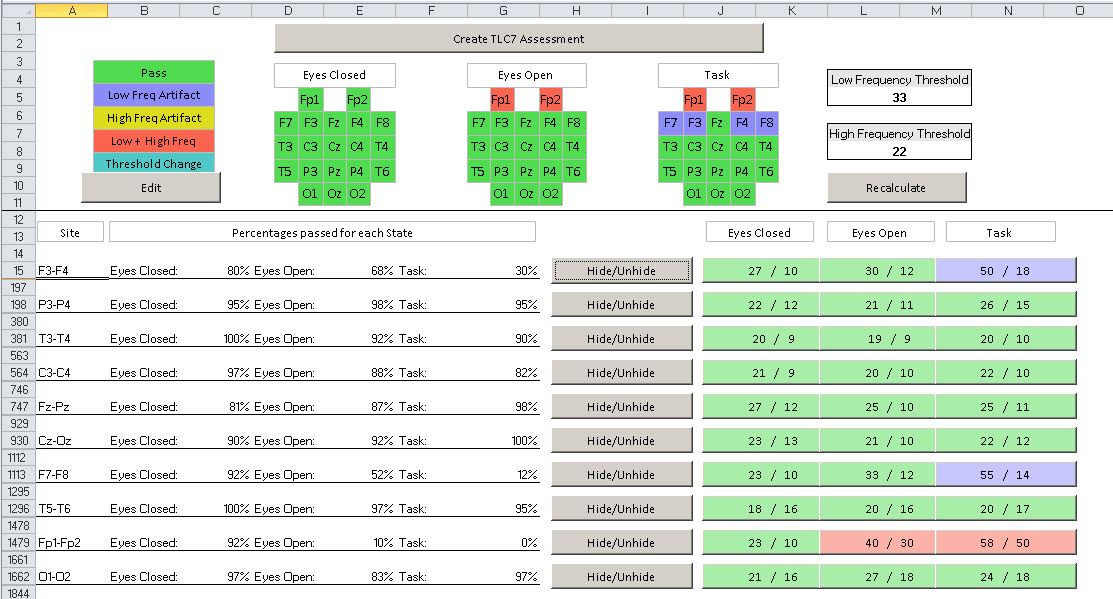
Look at the numbers in the buttons to the right of the page you sent. Each set of numbers are the cutoff values that would be required to 50+% of the seconds to pass. You can see that if the slow frequency cutoff were set at 65 (that’s the summed value of the 2 or 4 channels being recorded for 2-6 Hz activity) and the fast threshold were set at 27 (summed value of frequencies 23-42), all the sites that are currently green would pass. But even with the targets set 20% higher, at 77 and 33, none of the F3/F4 or P3/P4 sites pass. I assume you were recording 4C, so these were all recorded at the same time. I would suggest you go back and replay the .bxs recordings of several sites, including this one, and see if you don’t notice a difference. Is there a long bar at 60 hz? Is there a lot more surging? Is one side much more active than the other? It’s always a good idea to look carefully at the power spectrum and oscilloscope for a few seconds before starting to record; pause and reset the connections if necessary.
Each eye blink disrupts the signal for 2-4 seconds, and it’s not uncommon for people to blink 15-20 times a second. It’s crucial, if you want to get a good assessment, to minimize blinking and eye movement effects. While some people blink or shift their eyes a lot even with them closed, most do fine with EC. Asking the client to very lightly place the tip of the index finger on each eyelid during the EC recording can help in cases where uncontrolled EC eye movements are problem.
One last point: If I say that the best artifacting is done during recording, and if the auto-artifacting can usually do the most necessary cleaning when there isn’t major artifact, why bother to have the manual override that lets you change targets?
There are conditions like “hot temporals”, hot cingulate where fastwave activity is well out of normal range in an area; or white-matter head injuries with spikes of delta. Auto artifacting will screen these out as artifact–and letting that happen will reduce the accuracy and usefulness of the assessment. Adjusting the thresholds is critical, and that’s why you have that option.
No artifact in the record; no important data excluded from the record. That’s the goal.
Deciding which Data to Include or Exclude
Artifacting is a bit of an art, so it can seem confusing, but it’s also pretty common sense, which can make it quite simple.
The goal is to get as much useful information about the brain INTO the assessment without distorting it by including non-brain activity. The assessment shows you the maps for EC, EO and Task recordings, which ones passed (green)–meaning more than 30 seconds of good data were available, which ones didn’t and why. If the assessment is all green, which many are–and more as you get more experienced in recording–just accept it. If not, either reject it out of hand (obviously artifact) or look into and make a decision.
First Rule: If the heads are all blotched with colors, only 50 or 60% green, you either have a bad recording or a very difficult client. If the recording was bad, apologize and record again–better this time. If the client was bad, try some HEG and/or calming EEG protocols for 10 sessions. (May not even need to assess).
The best way to avoid artifact is not to record it. Watch the power spectrum to verify that the signals are symmetric. When they aren’t, re-prep the sites and try re-recording to see if the two sides are more alike. (Midline sites compare front with back of brain, so they may not be as symmetrical.) Verify that you are recording accurate brain patterns, then record.
Most often there will be a few blocks of color. Commonly they will be areas like F7/F8, F3/F4, Fp1/Fp2, sometimes Fz/Pz. Generally frontal sites, generally EO or at Task show eyeblink or eye-movement artifact in slow frequencies when the trainer and client don’t maintain focus on minimizing eye activity during recording. In most cases, I would agree with the program and exclude them.
Second Rule: Task data is nice, but it’s not strongly considered in training planning. Get in as much EC and EO data as possible without distorting the data.
Each site pair’s row beneath the graphs shows the percent of each state (EC/EO/TSK) that passed. Any value below 50% means that data won’t get into the assessment. If the pass percent is 47% or 39%, I’ll probably take a look at whether to revisit that ranking. If 47% is passing, then we only need 3% more to be able to use the data. 3% of 60 seconds is 1.8, so if I can change just 2 of the non-pass values to pass, we’ll be able to include those sites.
Clicking on the Hide/Unhide button, I can see the actual values for each second–the artifact in red. As I scan down the red numbers in the Slow column, I may see that the software set the threshold to 27u, and I find 3-4 values in the range from 27.1 to 30u. It’s doubtful that these are artifact–they’ll have a minor effect on the reported levels–and their addition will strengthen the completeness of the assessment.
The buttons to the right in each site pair’s row are a recent addition I asked for. They show the minimum artifact thresholds that would allow the site to pass. You can easily compare them against the thresholds in use (listed in the upper right). If my slow cutoff is set at 33, and I see that raising it to 39 would allow a site to pass, I’ll likely change it for the whole sheet to 39 (Recalculate).
But if I see that I’d have to change the cutoff to 48, that’s a much bigger jump. I might look deeper into the data, but in most cases I’d just exclude the site.
Artifacting Example
Our goal in the first phase of the assessment process is to get the clearest, most accurate, highest-resolution image of the brain’s activation patterns we can. That means removing as much artifact as we can. It also means NOT removing data that is likely to be good and important because we decide it’s artifact.
Hot temporal lobes or a hot cingulate or a delta spike related to a head injury can all cause significant false positives, tricking the auto-artifacting system. But those things, if they are NOT artifact, are important patterns in the brain we will want to train. Not allowing them in will reduce the effectiveness of the assessment.
When you look at the artifacting page, you see the selected threshold numbers for low frequency artifact (often related to eyeblinks, eye movement, cable movement, etc) and high frequency artifact (tension or movement). If you click on the Hide/Unhide button on any of the site-sets, you’ll see, in the first column, a list of epochs. 0-1 second, 1-2 seconds, etc. up to 179-180. The second column (Low Frequency) contains the sum of 2-4 Hz and 4-6 Hz activity in that second for all 4 sites. The third column (High Frequency) does the same for 23-38 and 38-42 Hz.
As you scroll down the list, you’ll see some rows red, others black.
Red rows are recommended for rejection as artifact based on the calculation of the spreadsheet. The number in the Low or High frequency column (or sometimes both) will be bold-faced, indicating that THIS was the number which exceeded the threshold and removed the data.
As you read across the top like with the sites identified, you can see the percent of sites that passed (neither slow nor fast frequency thresholds were exceeded in that second). I’m looking at a file in front of me, and I see a slow threshold of 33 (microvolts). The first rejected data line I see is because of a slow frequency vale of 35. Do I really think that second is artifact? I doubt it. It just got caught a little on the wrong side of the line.
Is it likely that either removing or including that line, with a value so close to the expected values will make a change in the final data–the average of all accepted sites? Very unlikely.
Now I scroll down further and suddenly I find a stretch of 9 seconds where the value goes from 37 all the way up by 79, with several reading in the mid-40’s and mid-50’s before ending with a 37. That sounds like a numerical representation of what I see on the power spectrum while recording an eye blink–all the slow frequencies surge out together and return together. Adding those values into the calculation of the average amplitude will make a noticeable difference, because there are a number of them and they are all well above the amplitudes before and after. I’ll leave them out.
You can go to that level of detail if it interests you, but there is also a quick and easy way on the artifacting page itself. Two numbers: the percent of seconds that passed in the area in question, and the “pass targets” listed to the right of each row.
If 43% passed, then I’d need to find another 7% (7%*60 seconds=4.2) 5 seconds of data that could be passed reasonably. If 14% passed, then I’ll need to find 23 seconds–a harder job. So the closer the pass % is to 50%, the easier it is to try to get in the data.
If the selected Thresholds are, say 33 for slow and 33 for fast, and the pass% numbers in the blue button not passing because of slow artifact are 50/18, then I would have to increase my low-frequency threshold by 50% (from 33-50). That’s a VERY big adjustment, and it would have a major effect on the values loaded into the assessment.
So now I have to ask myself whether there is a valid reason either for keeping the data out or adjusting to get it in.
I notice that 3 of the 4 sites not passing are Task recordings, and they are at F3/F4, F7/F8 and Fp1/Fp2–all very far frontal sites. The fourth site not passing is Fp1/Fp2 Eyes open. Eyes closed, all these sites look fine. Eyes open are okay except in the site closest to the eyes. Clients have the hardest time remembering their eye position when they are asked to perform a task (especially when, as at F7/F8 and Fp1/Fp2, the task involves using the eyes). It’s a pretty easy decision for me not to stretch the limits by 50% in order to pass data that I’m pretty positive are artifact.
But what if T3 and T4 aren’t passing because of high-frequency signals suspected of being artifact. If I know that when I recorded the sites I made sure the client let his mouth hang open–so there’s no bracing of the jaw muscles–and I noticed in watching the recording that there was significant fast activity, then I’m not so confident it’s artifact. After all, we have a category called “hot temporals” where these two sites (and/or with F7/F8 or T5/T6) have more fast activation than other brain sites.
If I see that I would have to raise the threshold from, say, 33 to 42 in order to pass it at least EC and EO data, I’d probably do it. I might also use the Hide/Unhide button to scroll down the data. If I find it runs within a range, maybe from 34-39u consistently, again, that doesn’t look like artifact. There’s no surging, no on/off. It’s just a more activated area.
There are some key assumptions built into the auto-artifacting procss:
1. That one set of targets for slow and fast activity (where artifacts are most likely to appear as surges in amplitude) can work for the whole brain. We tried setting thresholds for each site, but turned out badly. Key: remember that all the sites are compared against the same value, so a special site may show high levels of artifact which is really EEG.
2. Those targets are based on EC and EO parietal and central sites–areas where artifact is not easily produced. Obviously if recordings are bad at those sites, the targets may not be very useful, but if you can’t get good recordings in central and parietal, the whole assessment may be in question.
It’s important to remember that the most important thing you do in artifacting the file is record it properly. 90% of good artifacting is done in the recording process. DON’T LET ARTIFACT ENTER THE RECORDING. Then it’s easy to remove. If you keep the client still and relaxed (at least for 1 minute at a time) you’ll generally get all green when you process the data. Most of my experienced trainers send me files where there is no artifacting necessary beyond the automatic part. The file allows you to over-ride the automatic, and there are times you would want to do that, but it’s pretty simple to use.
Also important to remember that the goal of artifacting is not to get all the sites included in the assessment. It is to get all the sites and conditions included that provide clean brain data. Bad electrodes, poor connections, client movements and tension all can produce so much artifact or bad data that the file should NOT be included. Of course the trainer can keep adjusting the cutoffs until 50% of the data passes and the site/condition is included, but that will give an incorrect picture of the brain.
Usually the cutoffs are set based on P3/P4 and C3/C4, sites where it is not easy to produce artifact. If you have a site or condition that is blocked and showing a reasonable % of data passing with the existing cutoffs, then View that data. It’s not uncommon that, for example, the cutoff may be set at 44 and when you look at the data there are a number of values in the range from 44.1 to, say, 48. Those values are very close to the cutoff and unlikely are artifact, so you could adjust the cutoff to 48 without much danger of loading a bunch of artifact. If you have to adjust the cutoff to 65, then I would have some serious doubts.
Blinking
Anything you do as a task will likely have yes open and will likely involve moving them and probably will include blinking.
If you watch the replay of the recording, watch the power spectrum for surges where all slow activities go out and come back at once. In the oscilloscope, watch for big excursions in the baseline that look like an “S” tipped on its side.
Over-Artifacting
In the early-to-mid 90’s, when I was just starting off with an A620 amp, I was learning a lot from Joel & Judith Lubar, who were about 90 minutes away in Knoxville. We were using a 1C amp and software had been created for artifacting, which I was learning to use. Joel had showed it to me a month or so before, and he was in the office, sitting behind me as I started trying to look at each 2-second epoch and decide if it had artifact or not. After about 2 minutes of watching me obsess, Joel stood up to go, suggesting: Go through this one time as carefully as you can. Make sure you get every bit of artifact. Then go through it again and just take out the obvious stuff. See how they compare. I did so, and there was almost no difference at all. Serious muscle artifact or eye movement artifact make a clear excursion in the waveforms (or the power spectral displays. Just remove those and you’ll end up with a very good signal pretty quickly.
Slow and Fast-Wave Artifact
I worry about slow (eye movement/cable movement) and fast (muscle bracing or movements) artifacts. And I worry a lot more about those which are built in to the signal. If you can get a client to physically relax and be still for one minute at a time, you can remove artifact when there is a movement or tensing. But if the client is tense throughout, there’s no way to remove it. You get good recordings when you are recording–not when you are artifacting. If you are having to watch interocular tracings and EMG tracings, etc to see if the client is tense or blinking, you can’t be watching the one thing you really SHOULD be watching: the client.
Artifacting Recap
I think I’ve written about this before, but let me cover it again.
1. The goal of artifacting is to make sure that as little as possible of data that does not come from the brain gets into the assessment–AND that as little as possible REAL data is blocked from entering.
2. The best artifacting is done during the recording. Making sure that the client is “looking down” when recording frontal sites with EO or at task, making sure that the mouth is a bit open, so teeth can’t be clenched, are basic to getting a good recording. Watching the power spectrum display during the recording for places where the signal surges (either very slow frequencies–eye artifact–or all frequencies–often muscle) tells the trainer that artifact is occurring and how often. Ideally you pause and help the client get into the correct state for recording, or at least you know that a certain recording was bad.
3. When the auto-artifacting page shows problems, look at where they are. Fast artifact on the temporals can certainly be artifact–but if you paid attention during the recording, it’s probably not. We know that one important pattern of brain activity is “hot temporals”–where they are faster than the rest of the brain. They can fool the auto artifact routine. If you accept not passing the data, you are leaving out one of the most important training issues, so it won’t be a part of your plan. Same for alpha or delta spikes. Same for hot cingulate.
4. When in doubt, click the Hide/Unhide button in the row where the data are in question. Scroll down the list of 1-second epochs. The red ones are the ones that the algorithm accuses of being artifact, and when the number in the “fast” column is bold-faced red, it is what is blocking. If I see, for example, a target of 22 for fast activity, but in the temporals I consistently see red values that are in the low-to-middle 30’s (especially if I was watching when I recorded and saw that temporal lobe fast activity was greater than other areas without lots of surging), then I would believe the temporals were in fact hotter than the rest of the brain. I’d probably adjust my temporal lobe targets to pass the data. If, on the other hand, I see values surging 24, 31, 42, 58, 72, 128, 68, 49, etc., that looks a lot more like artifact, and I wouldn’t pass it.
5. If the required change in target for fast activity puts it around where the slow activity target is, (e.g. the targets are slow 33 and fast 22, and I have to change my fast target to 33 to pass the data, that eases my mind a bit more.
Threshold Changes for One Site or All
In most cases I prefer to use the same thresholds for all sites. However, if I see something like hot temporals, I may change only for the temporal lobes. Very rarely would I change just for one site and one condition.
TQ vs QEEG
I agree that Jay’s definition of QEEG is pretty clear and complete. It states:
Quantitative Electroencephalography (qEEG) is a procedure that processes the recorded EEG activity from a multi-electrode recording using a computer. This multi-channel EEG data is processed with various algorithms, such as the “Fourier” classically, or in more modern applications “Wavelet” analysis). The digital data is statistically analyzed, sometimes comparing values with “normative” database reference values. The processed EEG is commonly converted into color maps of brain functioning called “Brain maps”.
Various analytic approaches exist, from commercial databases to database free approaches, such as EEG phenotype analysis
The TQ7 processes multi-electrode recording using the fourier transform and converted into color maps and tables of brain functioning. Jay mentions phenotypes as an alternative to commercial databases, and that is exactly what the TQ7 uses. In fact I corresponded with him a decade or so ago, comparing his phenotypes with the TQ patterns, and we found they were almost exactly alike, though his do not give weight to the temporals, as the TQ does, and we don’t do a visual analysis of the raw EEG as he does.
Since our focus is on trainers, the TQ7 deals with what we find to be the most important issues to them:how all that analysis translates into actual training recommendations and how much of the increasingly limited resources of many real-world clients must be spent before beginning training. The whole-brain training plan works multiple patterns in a circuit, so we nearly always find that within the first five sessions one or more of these have had a positive response, reinforcing the client’s commitment to training. Also, since whole-brain training undoes the brain’s linked activation system from multiple points of view, it often produces a new stability within 2, 3 or 4 cycles. And it’s very hard to beat the cost–30 minutes of time with the same $4000 system that is used in training itself!
The population-based Q is essentially a research tool that gathers massive amounts of data about the brain and compares it against a normative database of people who were determined to have “normal” brains. If you understand statistical processing, you’ll understand that these readings were used to create a set of means and standard deviations for each age-group/sex combination, and these are used to produce what, for most people, is the most useful part of a QEEG report: the z-scores. These measure how many standard deviations each of the thousands of measures is from the mean for the comparison group. Of course it’s highly doubtful that ANY of the “normal” brains actually had low z-scores in all measures, so even “normal” brains are “abnormal” in some or many of the measures. Just looking at the z-scores, as some “readers” do, isn’t particularly helpful, since you need to know a good deal about brain function and expected patterns to be able to determine which, if any, of the z-score measures would actually be related to the real-world changes the client is seeking. You also need to be able to determine the difference between a “broken leg” and a “crutch”. One is a problem; the other is an adaptation to the problem, but both will appear as high z-scores. Training to get rid of the crutch may not be very helpful. Finally, you need to be comfortable with the whole idea of a “normal” brain. I like to ask people, “Do you really believe that a poet and an accountant will have the same brain?” If not, which one is normal? Norming is a useful concept in medicine and engineering that psychology has tried to apply to a field where it may make a lot less sense. Unlike, say, values for fasting blood sugar or other medical norms, there are multiple QEEG databases, and they don’t all agree on what is “normal”, so it’s important to know which one was used.
The TQ pattern-based QEEG, which you yourself could gather using the hardware and software (BioExplorer or Infiniti) you will use to train, is not normed. It is descriptive. It allows us to say whether a brain is fast or slow or fast in front and slow in back, etc. More importantly, it takes the results of many research studies done using QEEG to determining pattern analysis of various symptom constellations. You schedule an online meeting with someone from brain-trainer and go through what your TQ shows, what your training goals are, and why you are testing specific interventions.
When a person is highly anxious, for example, there are a number of EEG patterns which are very likely to appear in their brains that won’t appear in the brains of people who are not anxious. The brain-trainer system (the assessment and design package) is designed to guide you to protocols and sites that are likely to result in positive responses relative to the client’s desired changes. You usually get 3-6 “sessions” to test (where to place the electrodes and what patterns to train), one time each, to see what seems to have the greatest positive effect. Then you continue training that until it stabilizes.
If you purchased a Q, it would be fairly rare that it would not have come with some kind of reading and set of recommendations–often provided by someone other than the person who gathered the Q. Jay Gunkelman (qeegsupport.com) is probably among the most highly respected readers of Q’s. If I had to have a Q and have someone interpret it, I’d probably go to him, though there are many others in the field who are good as well.